Uterine
Fibroid
Introduction to Uterine Fibroid Embolization (UFE)
Tired of fibroids controlling your life? Heavy bleeding and pain don’t have to be your normal. At IR Clinic, our Uterine Fibroid Embolization (UFE) offers relief—a minimally invasive treatment that shrinks fibroids without surgery. Quick recovery. Effective results.
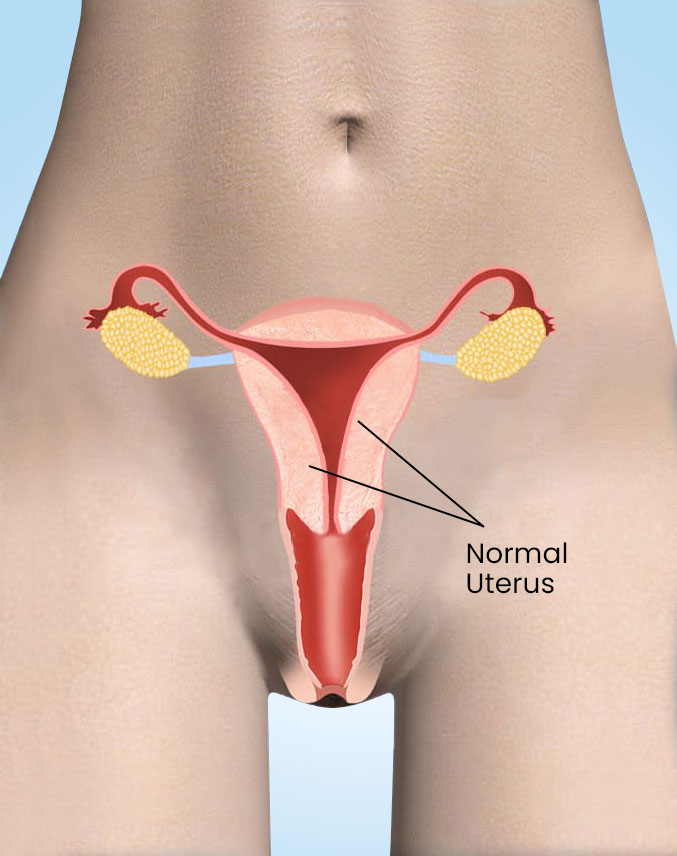
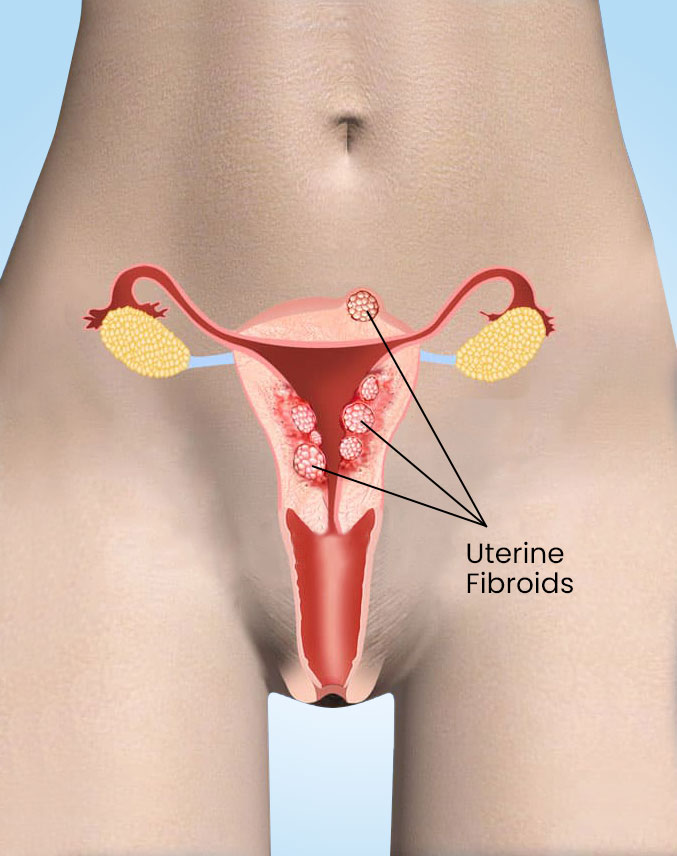
What are Uterine Fibroids?
Fibroids are noncancerous tumors made of smooth muscle and fibrous tissue that grow in the uterus. While 70–80% of women develop fibroids in their lifetime, not all experience symptoms or need treatment.
A key fact about fibroids is that they are almost always benign. Though some rare cases may begin as cancer, benign fibroids cannot turn cancerous. Because of this, many women without symptoms choose monitoring over treatment.
Fibroids vary in size—from as small as a pea to as large as a watermelon—and grow at different rates, even within the same woman. Regardless of size, effective treatment options are available to provide relief.
Who is at Risk for Uterine Fibroids?
While any woman can develop fibroids, certain factors significantly increase the risk. These influences range from unavoidable genetic predisposition to lifestyle choices that can be modified. Understanding these risk factors helps women assess their personal likelihood and take proactive steps when possible.
Aging
More common in women during their 30s–40s until menopause. Fibroids often shrink after menopause.
Family History
Having a close relative (like your mother) with fibroids triples your risk.
Ethnicity
African-American women develop fibroids at higher rates than white women.
Weight
Obesity increases risk, with severely overweight women facing 2–3x higher odds.
Diet
High red meat (beef, ham) consumption may raise risk, while green vegetables may help protect against fibroids.
What are The Symptoms of Fibroids?
While most fibroids cause no noticeable symptoms, about 30% of women with fibroids experience significant effects that may include:
- Heavy menstrual bleeding (may lead to anemia)
- Prolonged periods (lasting more than 7 days)
- Pelvic pressure or fullness (lower abdominal discomfort)
- Visible abdominal enlargement (may resemble pregnancy)
- Urinary frequency (due to bladder pressure)
- Painful intercourse (dyspareunia)
- Lower back or leg pain
- Pregnancy complications (including 6x higher C-section risk)
- Rare fertility issues (affecting conception in some cases)

How are Uterine Fibroids Diagnosed?
Fibroids are often first detected during a pelvic exam when your doctor feels an irregular uterine mass. To confirm the diagnosis, imaging tests are used.
Ultrasound is the most common initial test, using sound waves to create images of the uterus. It can be done abdominally or transvaginally for better detail. While quick and noninvasive, its accuracy depends on the operator’s skill.
For more detailed evaluation, an MRI provides clearer images, showing fibroid size, number, and location. It helps distinguish fibroids from similar conditions like adenomyosis and guides treatment decisions. Your doctor will recommend the best test based on your individual case.
How can Uterine Fibroids be Treated?
For women seeking alternatives to surgery, uterine fibroid embolization (UFE) offers an effective, minimally invasive treatment option. This interventional radiology procedure:
No
Surgery
Requires no surgical incisions, no scarring
Quick Procedure
Usually completed in under an hour
Faster Recovery
Require 1–2 week for recovery
Preserves Your Uterus
Targets only the fibroids
Image Guidance
Ensures safety and accuracy
Frequently Asked Questions (FAQs)
Avoid lifting more than 10 pounds for 48 hours. Strenuous exercise, including activities that increase blood flow to abdomen (some yoga positions) is discouraged for one week. If you work, arrange for two weeks of time off to allow complete recovery. Bathing: You may shower 24 hours after the procedure.
Most periprocedural complications are nonspecific to UFE and relate to vascular access and/or contrast agent use. These complications include arterial dissection, pseudoaneurysm, lower extremity emboli, puncture site hematoma, contrast allergy, contrast nephropathy, nerve injury, and infection.
UFE has been studied broadly by radiologists and gynecologists over the past 15 years. It resolves pain and bleeding 80 to 90% of the time. Fibroids will typically shrink 20 to 50% in the first 3 months and between 40 and 70% within a year.
Fibroid shrinkage after UFE begins immediately following treatment, but can continue for some time. Although some of your symptoms may resolve shortly after the UFE procedure, others can take months to improve.
Individual Response: Everyone's body responds differently to UFE. Some women may experience a significant reduction in abdominal size following the procedure, while others may see more modest changes.
Your doctor may suggest sleeping on your back or using a pillow or wedge to sleep on your side to increase your comfort.
The incidence of death following UFE is approximately 1 in 5,000-7,000 cases. One patient died from an infection that proceeded to sepsis and multi-organ system failure.
These risks include damage to the blood vessel, bruising or bleeding at the puncture site, and infection. The doctor will take precautions to mitigate these risks. There is always a chance that an embolic agent can lodge in the wrong place and deprive normal tissue of its oxygen supply.
Women diagnosed with uterine or endometrial cancer are not candidates for UFE, as the procedure is not designed to treat cancerous growths. In these cases, oncological treatment is the priority.
- Acute pain: The most common symptom of fibroids breaking down is a sharp pain in the abdomen that may be accompanied by swelling. ...
- Chronic pain: Some people experience less severe but longer-lasting pelvic pain.
- Fever: Fever can be a sign of fibroids breaking down.
Transient loss of periods may occur in 5 – 10% of patients after UFE. Younger patients tend to regain their period within six months. Ovarian failure resulting in menopause occurs in 1 – 3% of women younger than 40, but more frequently (7 – 14%) in women aged 45+.
Our fibroid embolization success rate means most of our patients who undergo the treatment report a reduction in symptoms, including the following:
- Shorter, lighter periods.
- Regular menstrual cycles.
- Resolution of anemia.
- Less pain during intercourse, if any.
- Normal urination and bowel movements.
- Less bloating, if any.
Although ischemia is the goal of the UFE procedure, ischemia also activates pain signals that respond to oxygen deficiency. This is thought to cause cramping pain at or around the site of treatment for a few days after the UFE procedure.
- Significantly shorter recovery times
- Less post-operative pain and scarring
- A lower risk of infection